How Semaglutide Suppresses Appetite: The Brain Science Behind GLP-1
Understanding how semaglutide suppresses appetite (not through willpower but through direct action on the brain's hunger-signaling pathways) explains why GLP-1 therapy produces results that lifestyle

In this article
Understanding how semaglutide suppresses appetite (not through willpower but through direct action on the brain's hunger-signaling pathways) explains why GLP-1 therapy produces results that lifestyle interventions alone rarely match.
*Compounded semaglutide is not FDA-approved. This article is for educational and informational purposes only and does not constitute medical advice. Clinical data referenced here reflects studies of FDA-approved pharmaceutical semaglutide unless otherwise noted. Individual results vary. Consult your licensed healthcare provider before starting, stopping, or adjusting any medication. Care at Prescriva is delivered by independently licensed providers, not by Prescriva LLC, which is a management services organization.*
---
Many people on semaglutide describe the same unexpected experience. They are not fighting the urge to eat through willpower. They simply do not feel hungry. Food they used to think about constantly just stops calling to them. The mental effort of dieting, the constant negotiation with cravings, seems to go quiet.
This is not a side effect. It is the mechanism. Semaglutide works primarily by changing how the brain interprets hunger signals. Understanding how it does this helps explain why the medication produces results that most lifestyle interventions alone cannot match, and why those results feel so different from calorie counting or conventional dieting.
Here is a clear explanation of the science.
---
What Is GLP-1 and Why Does It Matter for Appetite?
GLP-1 stands for glucagon-like peptide-1. Your body produces it naturally. Specialized cells in the small intestine called L-cells release GLP-1 into the bloodstream shortly after you eat, particularly in response to protein and fat. Once released, GLP-1 sends signals to the pancreas, the gut, and the brain.
In the pancreas, GLP-1 stimulates insulin release and suppresses glucagon, which helps regulate blood sugar. In the gut, it slows how quickly food moves from the stomach into the intestines. In the brain, it communicates that food has arrived, and that hunger should ease.
The problem is that your body's own GLP-1 works fast and breaks down quickly. The enzyme DPP-4 degrades natural GLP-1 within a few minutes. That means the satiety signal is brief, and for people prone to overeating or driven by strong food cravings, this signal is often not enough to overcome appetite.
Semaglutide is a GLP-1 receptor agonist: a compound engineered to mimic GLP-1 but resist enzymatic breakdown. It binds to the same receptors as your natural GLP-1, but its effects last for days rather than minutes. That extended duration allows it to maintain steady suppression of the hunger signals that natural GLP-1 can only briefly dampen.
---
How Semaglutide Acts on the Brain
The appetite-suppressing effects of semaglutide are not simply a downstream result of eating less. The medication reaches the brain directly and acts on the neural circuits that control hunger.
The Hypothalamus: Your Body's Appetite Thermostat
The hypothalamus is a small structure at the base of the brain. It serves as the body's central command for energy balance, regulating hunger, satiety, body temperature, and hormonal cycles. When it comes to appetite, the hypothalamus processes incoming signals from the gut, fat cells, and the bloodstream, then adjusts your drive to eat accordingly.
GLP-1 receptors are expressed throughout the hypothalamus, particularly in the arcuate nucleus - an area dense with neurons that promote feeding (AgRP neurons) and neurons that promote satiety (POMC neurons). When semaglutide binds to GLP-1 receptors in this region, it activates the satiety-promoting pathway and suppresses the hunger-promoting one.
A 2025 review in the *American Journal of Physiology - Cell Physiology* by Yada and colleagues examined GLP-1's role across the vagal afferents and hypothalamus in controlling feeding behavior (PMID [40241252](https://pubmed.ncbi.nlm.nih.gov/40241252/)). The researchers described how GLP-1 and the hunger hormone ghrelin work in opposite directions at these sites - GLP-1 signaling reduces food intake while ghrelin promotes it. Semaglutide, by sustained activation of GLP-1 receptors in these regions, shifts this balance toward satiety.
The Reward System: Turning Down the Volume on Food Cravings
The hypothalamus handles the mechanics of hunger. But many people do not overeat because they are physiologically starving. They overeat because food is rewarding - and the anticipation of that reward is hard to resist.
This is where the dopamine system comes in. Dopamine is the neurotransmitter most associated with pleasure and reward. The dopamine circuits in your brain evolved to drive you toward food, water, and other survival necessities. In a food-abundant modern environment, those circuits can be overactivated, producing cravings that have nothing to do with actual energy need.
A landmark 2025 study published in *Science* by Zhu and colleagues investigated exactly how GLP-1 receptor signaling interacts with the dopamine reward system (PMID [40146831](https://pubmed.ncbi.nlm.nih.gov/40146831/)). The researchers found that dopamine neurons in the reward circuits actively oppose GLP-1 receptor satiety signaling. When GLP-1R activation increased, these opposing dopamine neurons became less influential - meaning the rewarding pull of food felt less powerful. The researchers described this as a fundamental mechanism by which GLP-1R signaling reduces hedonic eating (eating for pleasure rather than hunger).
This provides a biological explanation for what many semaglutide users report: the medication does not just reduce physical hunger - it reduces the mental pull of food. The constant background noise of food thoughts quiets down.
---
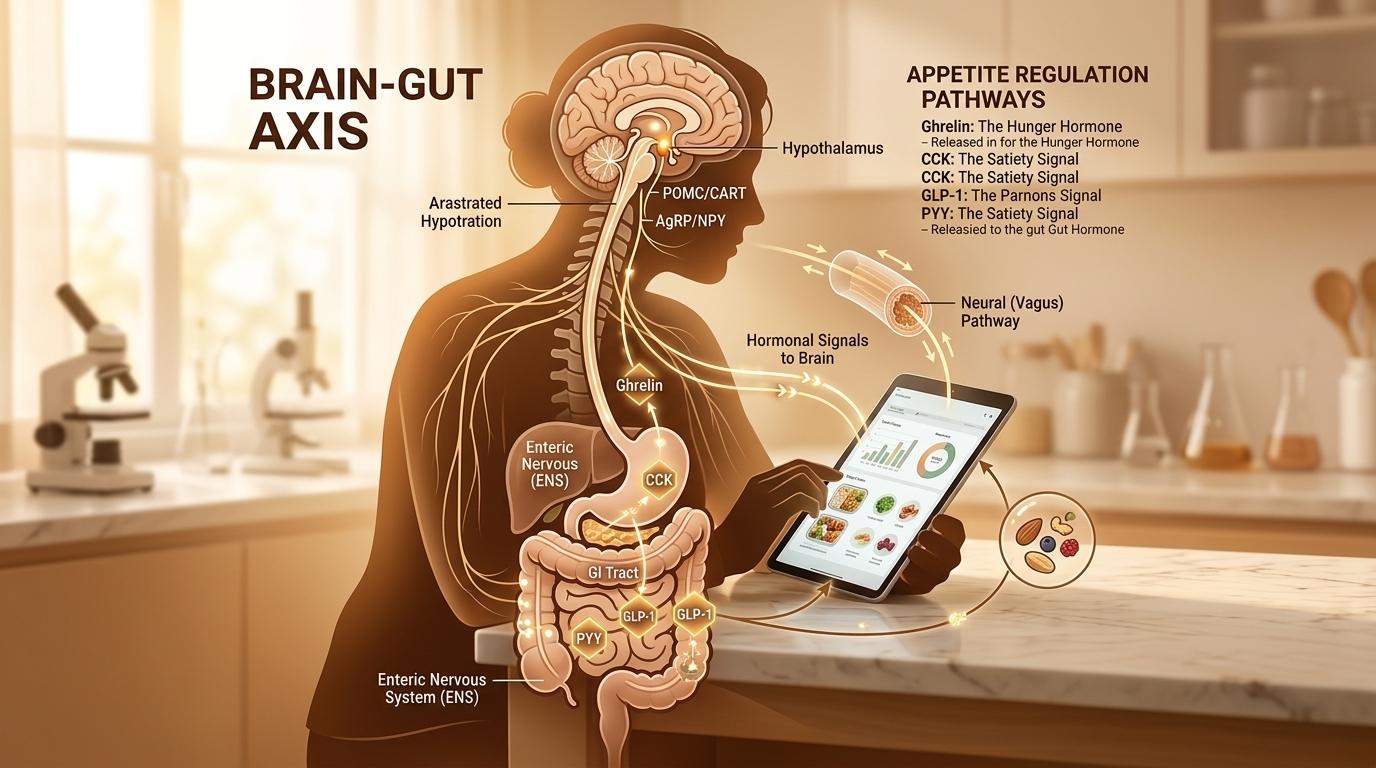
The Gut-Brain Axis: How the Body Signals the Brain
The brain does not work alone in regulating appetite. It receives a continuous stream of information from the gut, and GLP-1 plays a central role in that communication network.
Gastric Emptying: Staying Full Longer
One of semaglutide's clearest peripheral effects is slowing gastric emptying - the rate at which food leaves the stomach and enters the small intestine. A fuller stomach sends stretch signals to the vagus nerve, which the brain interprets as satisfaction. When food moves more slowly, those fullness signals last longer.
This effect contributes meaningfully to overall caloric reduction. When your stomach empties slowly, you feel satisfied after eating less, and you stay satisfied longer between meals. You are not suppressing an urgent hunger signal through discipline - the signal itself is muted.
The Vagus Nerve: Carrying Gut Signals to the Brain
The vagus nerve is the communication highway between the gut and the brain. It carries sensory information from the intestines, stomach, liver, and other organs upward to the brainstem and cortex. GLP-1 receptors are expressed on vagal sensory neurons, which means GLP-1 signals can travel this pathway to reinforce the central satiety message.
When semaglutide activates GLP-1 receptors both in the gut and the brain simultaneously - sustained over days rather than minutes - the overall effect on appetite is substantially greater than either pathway alone could achieve. The peripheral and central signals reinforce each other.
---
What Clinical Studies Show About Appetite and Food Behavior
The mechanistic picture is compelling. The clinical evidence is even clearer.
In a randomized clinical trial published in *Diabetes, Obesity and Metabolism*, Blundell and colleagues specifically studied how once-weekly semaglutide affected appetite, energy intake, and food preference in people with obesity (PMID [28266779](https://pubmed.ncbi.nlm.nih.gov/28266779/)). Using validated measures of appetite and carefully controlled food intake assessments, the researchers found that semaglutide reduced total caloric consumption, lowered hunger ratings, and reduced the desire to eat energy-dense foods. Participants reported less preoccupation with food - one of the clearest clinical signals of reduced hedonic drive.
A follow-up study by Gibbons and colleagues examined the effects of oral semaglutide on the same parameters in people with type 2 diabetes (PMID [33184979](https://pubmed.ncbi.nlm.nih.gov/33184979/)). The results were consistent: oral semaglutide reduced energy intake and improved appetite control compared to placebo. Participants ate less not because they were forcing themselves to, but because they genuinely wanted less food.
These findings connect directly to the large-scale weight loss outcomes seen in clinical trials. The STEP 1 trial, published in the *New England Journal of Medicine* by Wilding and colleagues, found that weekly semaglutide 2.4 mg produced a mean reduction of approximately 14.9 percent of body weight over 68 weeks in adults with obesity (PMID [33567185](https://pubmed.ncbi.nlm.nih.gov/33567185/)). That degree of weight loss reflects sustained reduction in caloric intake over more than a year - which is consistent with what the appetite and food preference data would predict.
---
Understanding "Food Noise"
Many people who use GLP-1 medications describe a phenomenon they call "food noise" - the constant mental background chatter about food. What to eat next. When you can have a snack. How much you could reasonably eat at dinner. For some people, this mental preoccupation runs nearly continuously.
On semaglutide, many users report that this noise goes quiet. They stop thinking about food between meals. The anticipation of eating loses its emotional weight. For people whose relationship with food has always been effortful and fraught, this experience can be genuinely surprising.
The Science study by Zhu et al. (PMID [40146831](https://pubmed.ncbi.nlm.nih.gov/40146831/)) provides a mechanistic basis for this. By reducing the influence of dopamine-driven reward signaling on feeding behavior, GLP-1 receptor activation appears to dial back the hedonic urgency that food normally carries. It does not remove the enjoyment of food entirely - most people still eat normally and enjoy meals - but it removes the compulsion that drives overconsumption.
A 2025 narrative review in the *International Journal of Molecular Sciences* also examined the neurobiological mechanisms behind GLP-1 receptor agonists and disordered eating patterns (PMID [41303457](https://pubmed.ncbi.nlm.nih.gov/41303457/)). The researchers noted that beyond simple appetite suppression, GLP-1R activation appears to modulate impulsivity and compulsive food-seeking behaviors, which may explain its relevance to a broader range of eating challenges than simple caloric restriction.
---
What Semaglutide Does Not Do
Setting accurate expectations matters. Semaglutide reduces appetite meaningfully, but it does not eliminate hunger entirely, nor does it remove all enjoyment of food. Most people still eat regular meals - they simply eat less, feel satisfied more easily, and think about food less between meals.
The medication also does not replace nutrition principles. Protein intake remains important for preserving lean muscle mass during weight loss. Vegetables, fiber, and balanced meals support the metabolic changes the medication initiates. The medication creates the physiological conditions for easier caloric reduction; how you eat within that window still shapes your outcomes.
Semaglutide's appetite-suppressing effects are most pronounced in the first months of treatment and may moderate somewhat over time as the body adapts. Regular communication with your provider about dosing and your experience helps optimize the balance between efficacy and [side effects](/resources/semaglutide-side-effects-what-to-expect).
---
A Note on Compounded Semaglutide
The studies referenced in this article used FDA-approved pharmaceutical semaglutide. Compounded semaglutide is a different product - prepared by licensed 503A compounding pharmacies based on individual prescriptions. Compounded semaglutide is not FDA-approved, and the efficacy and safety data from branded drug trials cannot be directly attributed to compounded formulations.
This distinction matters for accurate understanding of what the evidence does and does not show.
---
The Bigger Picture
For decades, weight management was framed primarily as a behavioral problem. Eat less. Move more. Choose discipline over impulse. This framing ignored the biology underneath those impulses - the hormonal signals, neural circuits, and neurochemical systems that powerfully drive food-seeking behavior.
Semaglutide does not work by giving you more willpower. It works by changing the signals your brain receives. The hypothalamus gets a sustained satiety message. The dopamine reward circuits register food as less urgently rewarding. The stomach empties more slowly, extending fullness. The vagus nerve carries those signals upward continuously.
The result is that eating less becomes, for many people, significantly easier - not because they are trying harder, but because the biological pressure driving overconsumption has been reduced.
Understanding this mechanism helps explain both why the medication works when it does, and what to expect from it. It is not magic, and it is not just appetite suppression. It is a meaningful recalibration of the systems that regulate how you experience hunger.
---
Ready to Explore Your Options?
If you are considering a medically supervised weight management program, we can help you understand whether you qualify and what the process looks like. [Check your eligibility](/assessment) and speak with a licensed provider to learn more.
*This is not medical advice. Results vary. Compounded semaglutide is not FDA-approved. Consult your healthcare provider before starting any medication.*
---
Sources
- Wilding JPH, Batterham RL, Calanna S, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity. *N Engl J Med.* 2021;384(11):989-1002. PMID: [33567185](https://pubmed.ncbi.nlm.nih.gov/33567185/)
- Blundell J, Finlayson G, Axelsen M, et al. Effects of once-weekly semaglutide on appetite, energy intake, control of eating, food preference and body weight in subjects with obesity. *Diabetes Obes Metab.* 2017;19(9):1242-1251. PMID: [28266779](https://pubmed.ncbi.nlm.nih.gov/28266779/)
- Gibbons C, Blundell J, Tetens Hoff S, et al. Effects of oral semaglutide on energy intake, food preference, appetite, control of eating and body weight in subjects with type 2 diabetes. *Diabetes Obes Metab.* 2021;23(2):581-588. PMID: [33184979](https://pubmed.ncbi.nlm.nih.gov/33184979/)
- Zhu Z, Jiang Y, et al. Hedonic eating is controlled by dopamine neurons that oppose GLP-1R satiety. *Science.* 2025 Mar 28. PMID: [40146831](https://pubmed.ncbi.nlm.nih.gov/40146831/)
- Yada T, Yanagi A, Sugino S. GLP-1 and ghrelin inversely regulate insulin secretion and action in pancreatic islets, vagal afferents, and hypothalamus for controlling glycemia and feeding. *Am J Physiol Cell Physiol.* 2025 Jun 1. PMID: [40241252](https://pubmed.ncbi.nlm.nih.gov/40241252/)
- Tongta S, Davenport AP. Neurobiological Mechanisms and Therapeutic Potential of Glucagon-like Peptide-1 Receptor Agonists in Binge Eating Disorder: A Narrative Review. *Int J Mol Sci.* 2025 Nov 13. PMID: [41303457](https://pubmed.ncbi.nlm.nih.gov/41303457/)
Stay informed
Weekly research updates and health guides. No spam.
References
- Wilding JPH, Batterham RL, Calanna S, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity. N Engl J Med. (2021).
- Blundell J, Finlayson G, Axelsen M, et al. Effects of once-weekly semaglutide on appetite, energy intake, control of eating, food preference and body weight in subjects with obesity. Diabetes Obes Metab. (2017).
- Gibbons C, Blundell J, Tetens Hoff S, et al. Effects of oral semaglutide on energy intake, food preference, appetite, control of eating and body weight in subjects with type 2 diabetes. Diabetes Obes Metab. (2021).
- Zhu Z, Jiang Y, et al. Hedonic eating is controlled by dopamine neurons that oppose GLP-1R satiety. Science. (2025).
- Yada T, Yanagi A, Sugino S. GLP-1 and ghrelin inversely regulate insulin secretion and action in pancreatic islets, vagal afferents, and hypothalamus for controlling glycemia and feeding. Am J Physiol Cell Physiol. (2025).
- Tongta S, Davenport AP. Neurobiological Mechanisms and Therapeutic Potential of Glucagon-like Peptide-1 Receptor Agonists in Binge Eating Disorder: A Narrative Review. Int J Mol Sci. (2025).
Ready to get started?
Check if you qualify for a personalized treatment plan.
Check Your Eligibility →Continue reading

GLP-1 Medications After Bariatric Surgery: What the Research Shows About Weight Regain

Tirzepatide and Birth Control: What You Need to Know About Oral Contraceptives
