GLP-1 Medications and the Gut-Brain Axis: The Science of Why You Feel Full
If you have ever wondered why GLP-1 medications work so differently from a traditional "eat less, move more" approach, the answer lives in a communication network connecting your gut and your brain. T

In this article
*Compounded semaglutide and compounded tirzepatide are not FDA-approved. This article is for educational and informational purposes only and does not constitute medical advice. Clinical data referenced here reflects studies of GLP-1 receptor agonists as a medication class unless otherwise noted. Individual results vary. Consult your licensed healthcare provider before starting, stopping, or adjusting any medication or treatment plan. Care at Prescriva is delivered by independently licensed providers, not by Prescriva LLC, doing business as Prescriva, which is a management services organization.*
---
If you have ever wondered why GLP-1 medications work so differently from a traditional "eat less, move more" approach, the answer lives in a communication network connecting your gut and your brain. This network, called the gut-brain axis, is why many people on GLP-1 therapy report feeling satisfied after smaller portions without consciously trying to restrict themselves.
This is not about willpower. It is about biology.
What Is the Gut-Brain Axis?
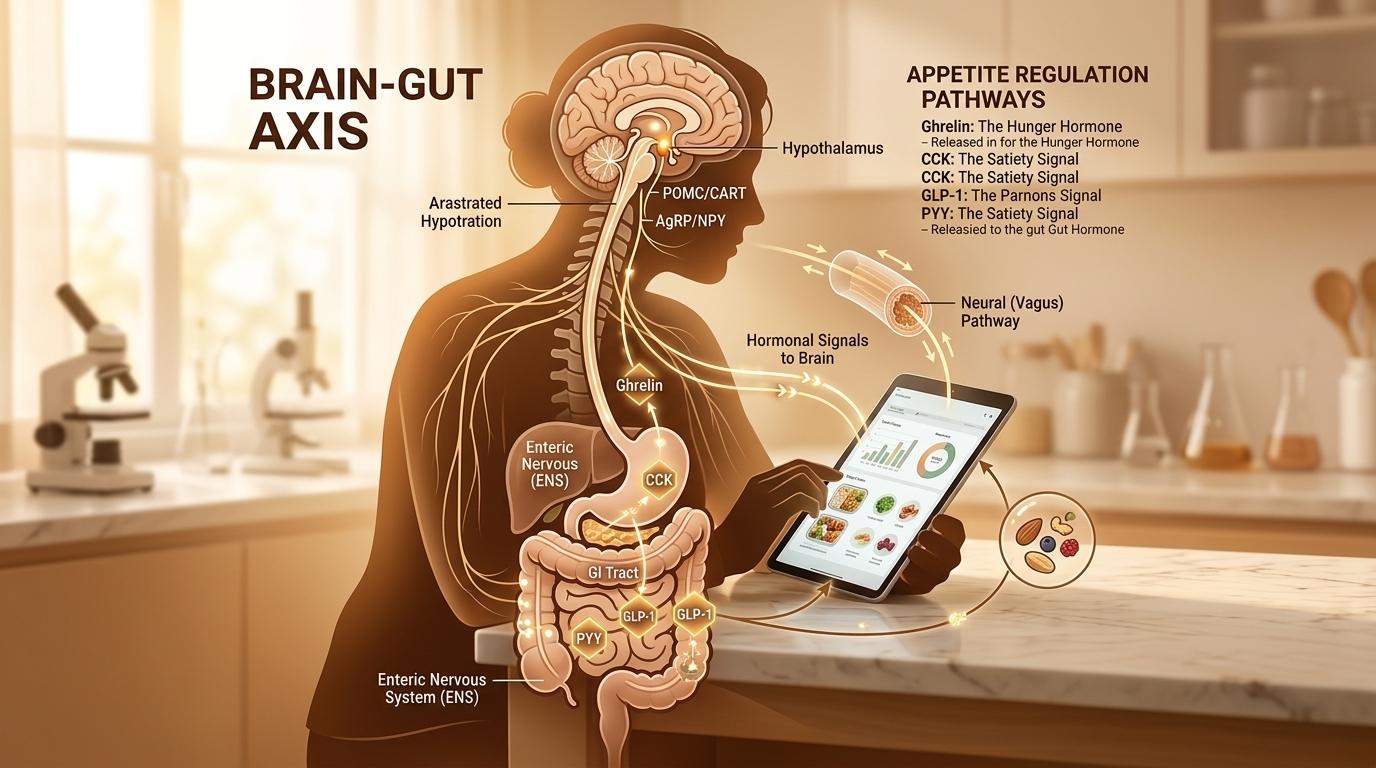
Your gut and your brain are in constant communication. The vagus nerve, a long cranial nerve that runs from the brainstem down through the chest and abdomen, carries signals in both directions. Your gut sends hormonal and neural messages upward toward the brain, reporting on what you have eaten, how full the stomach is, and what nutrients have been absorbed.
This bidirectional highway is the gut-brain axis. It influences hunger, appetite, mood, and even how your body stores energy. Research published in *Nature Reviews Endocrinology* describes this system as fundamental to energy homeostasis, the biological process that keeps your body weight relatively stable over time. (Andersen et al., PMID: 29728598)
When the system is working normally, your gut tells your brain when you have eaten enough. The brain processes those signals and generates the feeling of fullness. When this feedback loop is disrupted, which can happen through chronic overeating, high-fat diets, and metabolic changes, the fullness signal becomes delayed or muted. (Al Helaili et al., PMID: 32943186)
GLP-1 receptor agonists work, in part, by restoring and amplifying this signal.
How Your Body Makes GLP-1 Naturally
Glucagon-like peptide-1, or GLP-1, is a hormone your intestine produces in response to eating. Specialized cells called L-cells, which line the walls of your small intestine and colon, detect nutrients as food passes through. When they sense carbohydrates, fats, and proteins, they release GLP-1 into the bloodstream.
GLP-1 then travels to the pancreas, where it stimulates insulin release (only when blood sugar is elevated, which limits hypoglycemia risk), and to the brain, where it signals fullness. Research published in *Frontiers in Nutrition* identifies L-cells as central players in appetite regulation, acting as nutrient sensors that translate the contents of your gut into hormonal signals your brain can read. (Spreckley et al., PMID: 26258126)
The challenge is that native GLP-1 breaks down very quickly in the bloodstream, within minutes. The enzyme DPP-4 degrades it before it can act for long. This is why eating a meal generates a fullness signal, but why that signal fades relatively quickly.
The Vagal Nerve: Your Gut-to-Brain Superhighway
Before GLP-1 even reaches the brain through the bloodstream, some of its effects are transmitted neurally. GLP-1 receptors are expressed on vagal afferent neurons, the nerve fibers that carry sensory information from the gut upward to the brainstem.
When L-cells release GLP-1 after a meal, it activates these vagal receptors, which then send electrical signals directly to a region of the brainstem called the nucleus tractus solitarius (NTS). The NTS is a key integration center for satiety signals. It processes information from the gut and relays it to the hypothalamus, the brain region that governs hunger and energy balance.
A 2024 study published in *Nature* found that distinct GLP-1 receptor circuits in the hindbrain separately regulate satiety (feeling full and satisfied) and aversion (nausea and discomfort), offering important insight into how the medication's effects on appetite can be separated from its side effects. (Huang et al., PMID: 38987598)
This neural pathway works faster than hormonal signaling through the bloodstream. It is one reason why the effects of GLP-1 receptor agonist medications can begin shaping eating behavior before drug levels in the blood reach peak concentration.
How GLP-1 Receptor Agonists Amplify This System
GLP-1 receptor agonists are a class of medications designed to mimic and prolong the action of native GLP-1. Where natural GLP-1 is degraded in minutes, these medications are engineered to resist that breakdown and remain active for hours or days depending on the formulation.
By maintaining elevated GLP-1 receptor activation over a sustained period, these medications effectively extend and amplify the satiety signal your body would normally generate briefly after eating.
Research published in *Molecular Metabolism* by Drucker, one of the leading researchers in incretin biology, describes how GLP-1 receptor agonists act at multiple levels of the gut-brain axis simultaneously: stimulating peripheral vagal neurons, activating brainstem circuits, and directly engaging hypothalamic neurons that control food intake. (Drucker, PMID: 34626851)
The result is a stronger, longer-lasting experience of fullness. Many people describe this as "food noise" becoming quieter, meaning the persistent mental preoccupation with food and eating diminishes. This is not suppressing hunger through stimulant-type mechanisms. It is reinforcing the body's natural satiety biology.
Compounded semaglutide and compounded tirzepatide are GLP-1 receptor agonists prescribed through Prescriva's provider network. They are not FDA-approved as compounded formulations. They are prescribed by independently licensed healthcare providers after individual medical evaluation.
Gastric Emptying: Why Food Stays With You Longer
One of the gut-level mechanisms that reinforces the fullness signal is slowed gastric emptying. GLP-1 receptor activity slows the rate at which your stomach empties its contents into the small intestine.
This has two effects. First, the stomach remains fuller for longer after a meal, contributing to physical feelings of satiety. Second, nutrients arrive in the intestine more gradually, which blunts the post-meal glucose spike and extends the window during which L-cells are releasing satiety hormones.
Research on GLP-1 biology and the incretin system describes gastric emptying effects as one of the primary peripheral mechanisms through which GLP-1 receptor agonists reduce caloric intake. (Baggio et al., PMID: 17498508)
It is worth noting that this gastric slowing is also responsible for some of the nausea that some people experience early in treatment, particularly during dose escalation. The sensation of nausea typically diminishes as the body adapts.
The Hypothalamus: Where Hunger Decisions Are Made
Once gut signals reach the brainstem, they continue upward to the hypothalamus. Two regions within the hypothalamus are especially important for appetite regulation. The arcuate nucleus contains neurons that either stimulate hunger (AgRP/NPY neurons) or suppress it (POMC neurons). GLP-1 receptor activation shifts the balance toward the suppressive POMC neurons.
A 2023 review in *Trends in Pharmacological Sciences* describes GLP-1 receptor agonists as operating on these hypothalamic circuits in ways that are distinct from older weight-loss medications that targeted reward pathways or stimulant pathways. The result is a physiologically grounded reduction in drive to eat, rather than a pharmacological override of normal brain function. (Boer et al., PMID: 36462999)
The hypothalamus also integrates GLP-1 signaling with other metabolic hormones, including leptin (the hormone secreted by fat cells to signal energy sufficiency) and ghrelin (the hunger hormone released by an empty stomach). In obesity, leptin resistance is common, meaning the brain stops responding appropriately to leptin's "you have enough stored energy" signal. GLP-1 receptor agonists appear to work partly by bypassing or supplementing this disrupted signaling, providing a more direct satiety input to the hypothalamus.
Beyond Hunger: Reward, Cravings, and Food Choices
The gut-brain axis also connects to the brain's reward system. GLP-1 receptors are expressed in the ventral tegmental area and nucleus accumbens, regions associated with dopamine-driven reward and motivation.
This may help explain why some people on GLP-1 therapy report changes in their relationship with highly palatable foods, noting less drive to seek out sweets or high-calorie snacks. Research on GLP-1 and neuroinflammation published in *Pharmacological Research* notes that GLP-1 receptors in reward circuits may modulate the motivational salience of food-related cues. (Kopp et al., PMID: 36372278)
This does not mean GLP-1 therapy removes enjoyment of food. Most people continue to enjoy eating. What changes is the compulsive quality that can drive overeating in some individuals. Food choices tend to shift not because of conscious discipline, but because the neurological drive to overconsume high-reward foods decreases.
What This Means for Your Weight Loss Journey
Understanding the gut-brain axis helps reframe what GLP-1 therapy actually does. It is not suppressing your appetite through force. It is restoring and amplifying the biological signaling your body was already designed to use.
For many people, years of consuming highly processed, calorie-dense foods have blunted these natural satiety signals. GLP-1 receptor agonists essentially turn the volume back up on a system that was never intended to stay quiet.
A few practical implications of this biology:
Smaller portions feel sufficient. Because gastric emptying slows and satiety signals strengthen, finishing a smaller meal often produces genuine satisfaction rather than the frustrated, still-hungry feeling that comes with calorie restriction alone.
Meal pacing matters. Since the gut-brain axis operates with a slight delay (it takes about 20 minutes for satiety signals to peak after eating begins), eating more slowly allows those signals to catch up before you overshoot.
Protein supports the system. L-cells respond strongly to protein in the gut. Meals higher in protein stimulate more robust GLP-1 release and tend to produce greater satiety per calorie than meals dominated by refined carbohydrates.
Individual response varies. Factors including gut microbiome composition, prior dietary history, vagal tone, and genetics all influence how strongly any individual responds to GLP-1 therapy. This variability is normal and is one reason medical supervision matters.
Frequently Asked Questions
Does GLP-1 therapy permanently change how the gut-brain axis works?
Research does not yet support the idea of permanent changes. Most evidence suggests that the effects on satiety signaling are active during treatment. Long-term benefits depend on concurrent lifestyle changes in diet and physical activity that support sustainable weight management.
Can the gut-brain axis be supported without medication?
Yes. High-fiber diets, probiotic-rich foods, regular physical activity, and adequate sleep all support healthy gut-brain communication. For people with significant metabolic disruption, however, lifestyle approaches alone may not be sufficient to overcome resistance in the satiety signaling system. This is where GLP-1 receptor agonist therapy, under medical supervision, can help restore normal signaling.
Is this why GLP-1 medications cause nausea?
Partly. The same vagal and brainstem circuits that carry satiety signals also carry signals associated with nausea. The hindbrain circuits for fullness and nausea partially overlap, which is why stimulating satiety pathways, especially at higher doses, can produce nausea as a side effect. Most people find nausea decreases as their body adjusts to the medication. (Huang et al., PMID: 38987598)
The Bottom Line
GLP-1 medications work because they speak the body's own language. Your gut has always been designed to send fullness signals to your brain. GLP-1 receptor agonists extend the duration and strength of those signals, helping the brain receive the "enough" message more clearly.
This science does not mean the medications do all the work. Diet quality, physical activity, sleep, and stress management all influence how well the gut-brain axis functions and how sustainable your results will be. GLP-1 therapy works best as part of a medically supervised program that addresses these factors together.
If you are wondering whether GLP-1 therapy might be right for you, Prescriva's licensed providers can evaluate your history, answer your questions, and help you understand what a supervised treatment plan would look like.
*Individual results vary. This article does not constitute medical advice. Compounded semaglutide and compounded tirzepatide are not FDA-approved. Consult your healthcare provider before starting any medication.*
---
References
- Andersen A, et al. "Glucagon-like peptide 1 in health and disease." *Nature Reviews Endocrinology*. 2018. PMID: [29728598](https://pubmed.ncbi.nlm.nih.gov/29728598/)
- Spreckley E, Murphy KG. "The L-Cell in Nutritional Sensing and the Regulation of Appetite." *Frontiers in Nutrition*. 2015. PMID: [26258126](https://pubmed.ncbi.nlm.nih.gov/26258126/)
- Huang Y, et al. "Dissociable hindbrain GLP1R circuits for satiety and aversion." *Nature*. 2024. PMID: [38987598](https://pubmed.ncbi.nlm.nih.gov/38987598/)
- Drucker DJ. "GLP-1 physiology informs the pharmacotherapy of obesity." *Molecular Metabolism*. 2022. PMID: [34626851](https://pubmed.ncbi.nlm.nih.gov/34626851/)
- Boer GA, Holst JJ. "Obesity pharmacotherapy: incretin action in the central nervous system." *Trends in Pharmacological Sciences*. 2023. PMID: [36462999](https://pubmed.ncbi.nlm.nih.gov/36462999/)
- Baggio LL, Drucker DJ. "Biology of incretins: GLP-1 and GIP." *Gastroenterology*. 2007. PMID: [17498508](https://pubmed.ncbi.nlm.nih.gov/17498508/)
- Al Helaili A, et al. "Chronic high fat diet impairs glucagon like peptide-1 sensitivity in vagal afferents." *Biochemical and Biophysical Research Communications*. 2020. PMID: [32943186](https://pubmed.ncbi.nlm.nih.gov/32943186/)
- Kopp KO, et al. "Glucagon-like peptide-1 (GLP-1) receptor agonists and neuroinflammation." *Pharmacological Research*. 2022. PMID: [36372278](https://pubmed.ncbi.nlm.nih.gov/36372278/)
Stay informed
Weekly research updates and health guides. No spam.
References
- Andersen A, et al. "Glucagon-like peptide 1 in health and disease." *Nature Reviews Endocrinology*. 2018. PMID: 29728598. Published Research (2018).
- Spreckley E, Murphy KG. "The L-Cell in Nutritional Sensing and the Regulation of Appetite." *Frontiers in Nutrition*. 2015. PMID: 26258126. Published Research (2015).
- Huang Y, et al. "Dissociable hindbrain GLP1R circuits for satiety and aversion." *Nature*. 2024. PMID: 38987598. Published Research (2024).
- Drucker DJ. "GLP-1 physiology informs the pharmacotherapy of obesity." *Molecular Metabolism*. 2022. PMID: 34626851. Published Research (2022).
- Boer GA, Holst JJ. "Obesity pharmacotherapy: incretin action in the central nervous system." *Trends in Pharmacological Sciences*. 2023. PMID: 36462999. Published Research (2023).
- Baggio LL, Drucker DJ. "Biology of incretins: GLP-1 and GIP." *Gastroenterology*. 2007. PMID: 17498508. Published Research (2007).
- Al Helaili A, et al. "Chronic high fat diet impairs glucagon like peptide-1 sensitivity in vagal afferents." *Biochemical and Biophysical Research Communications*. 2020. PMID: 32943186. Published Research (2020).
- Kopp KO, et al. "Glucagon-like peptide-1 (GLP-1) receptor agonists and neuroinflammation." *Pharmacological Research*. 2022. PMID: 36372278. Published Research (2022).
Ready to get started?
Check if you qualify for a personalized treatment plan.
Check Your Eligibility →

